
By Anissa Durham | Word In Black
(WIB) – At 40 weeks pregnant, Georgina Dukes-Harris drove to her weekly OB-GYN appointment in Clemson, South Carolina. It was 8 a.m. on Dec. 14, 2011. The doctor told her there’s no need for her son to “bake any longer.” So, the first-time mom returned, as instructed, at 6 p.m. on the same day. Health care providers gave her Pitocin to induce labor.
Next, they gave her an epidural and broke her water. Dukes-Harris was now on a time clock. She had 48 hours to give birth before complications could set in for her and the baby. Even though her cervix wasn’t fully dilated to 10 centimeters, doctors told her to push.
Four to five hours of pushing and nothing was happening.
“I was pushing, and they used forceps to try to pull him out, and it left a big scar on his head.” she says, “It’s like I had two births in one.”
At that point, Dukes-Harris’ heart rate spiked, and the baby showed signs of distress. Doctors decided to give her an emergency C-section on Dec. 16, which she describes as a deeply traumatic experience.
At 19-years-old and in the best shape of her life, Dukes-Harris recalls following her doctors’ instructions to a T. But the trauma that came with her unplanned C-section left her dealing with postpartum depression and anxiety for more than a year afterward.
Dukes-Harris’s story is one of many that highlight the challenges Black birthing people face in America. Maternal care deserts, abortion bans, and the overutilization of C-section have all traumatized and even ended the lives of Black women. Now Black birthing people, physicians, and holistic care providers are pushing for a more patient-centered approach.
Black Mothers Face Higher Risks and Limited Options
 A 2024 March of Dimes report found that 35% of U.S. counties are maternity care deserts, which are counties with no birthing facilities or obstetric clinicians. Chronic conditions related to poor health outcomes for birthing people like pre-pregnancy obesity, hypertension, and diabetes have increased since 2015 and are most common in maternity care deserts. These conditions are also most common among Black and American Indian and Alaska Native birthing people.
A 2024 March of Dimes report found that 35% of U.S. counties are maternity care deserts, which are counties with no birthing facilities or obstetric clinicians. Chronic conditions related to poor health outcomes for birthing people like pre-pregnancy obesity, hypertension, and diabetes have increased since 2015 and are most common in maternity care deserts. These conditions are also most common among Black and American Indian and Alaska Native birthing people.
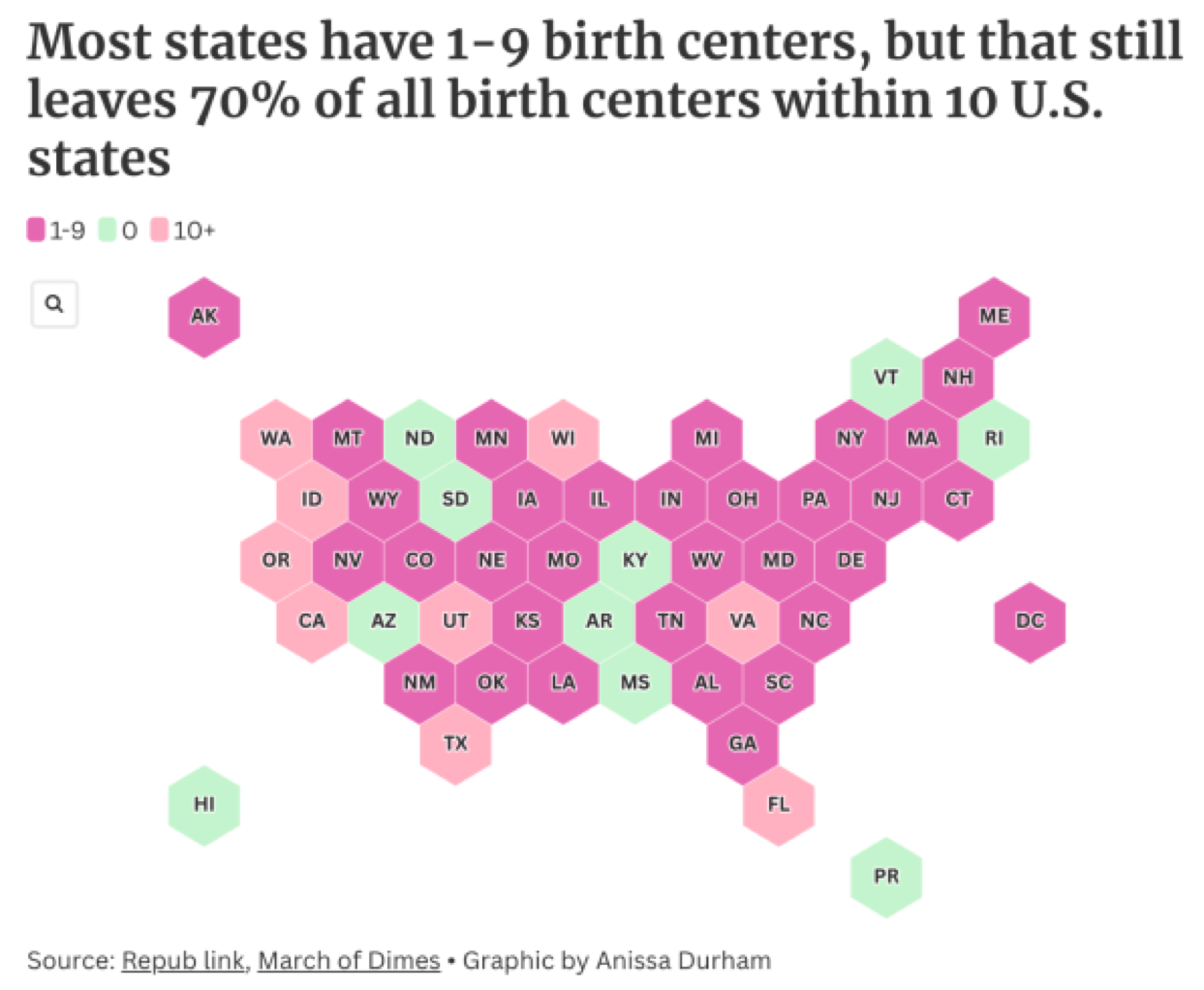
Pregnant people who give birth in counties that are identified as maternity care deserts or low access areas have poorer health before pregnancy, receive less prenatal care, and experience higher rates of preterm births. Most states have between one and nine birth centers, but that still leaves 70% of all birth centers residing within 10 states.
“We serve four different counties that do not have any OB-GYNs at all,” says Joy Baker, an OB-GYN in LaGrange, Georgia. “The real issue is these are communities that already have diminished access to social determinants of health … I think of them as political determinants of health. These places don’t become under resourced by accident.”
Barriers to Maternal Health Care
Pregnant people in areas identified as maternity care deserts often travel between 26 to 38 minutes for obstetric care. During pregnancy and childbirth, longer travel time is associated with higher risk of maternal morbidity, stillbirth, and neonatal intensive care unit admission, the report states. And Black women are already at a higher risk for gestational diabetes, preeclampsia, and postpartum hemorrhage.
“There’s not one condition that I can think of that gets better in pregnancy,” Baker says. “It’s usually exacerbated.”
Now, more than two years after fact, the overturn of Roe v. Wade, the landmark decision that protected a women’s right to an abortion, has complicated things for physicians like Baker. In Southern states with some of the strictest abortion bans like Georgia, Louisiana, Mississippi, and South Carolina, Black women are facing more barriers to access reproductive health care.
But it’s not just patients who are struggling.
Each state has a different abortion ban or restriction, often making it unclear as to what a physician is able to do. For example, in Georgia, abortion is restricted to six weeks or less. Although the law has exceptions to protect the “life of the mother,” the language is vague and can leave loopholes for doctors to be prosecuted if a physician intervenes too early.
In Baker’s personal practice, she hasn’t been affected too much by the abortion bans. But she says there are physicians in neighboring counties that have struggled with caring for their patients due to the law.
“Doctors are afraid. When you have spent your entire life training and building a career, the last thing you want is to go to prison for just doing your job,” Baker says. “There is a lot of fear surrounding that. It’s been horrible to the physician patient relationship.”
Birthing Shouldn’t Be Traumatic

Courtesy of Lauren Elliot.
At 38 weeks pregnant, Lauren Elliot’s doctor told her the umbilical cord was wrapped around her son’s neck at least three times. Later, they realized it was wrapped around his neck five times. Delivering vaginally no longer became an option when her son was in distress. Elliot, 29 at the time, had a C-section.
“I was paralyzed with emotion from wanting him to be OK,” she says.
Shortly afterward she developed postpartum preeclampsia. And like Dukes-Harris, Elliot, now 36, described a C-section as a traumatic experience. Although her son was delivered healthy, the mental health toll from her first birthing experience loomed over her for two years. She struggled with anxiety and panic attacks. To cope she created Candlelit Care, an app-based behavioral health clinic that supports Black birthing people throughout a pregnancy and afterwards.
For her next pregnancy, Elliot determined to have a vaginal birth after a cesarean section or VBAC. But many doctors worry about a uterine rupture even if a patient has fully healed from a C-section. She also made the intentional decision to have a Black OB-GYN.
But even that wasn’t enough.
During labor with her second child, Elliot wasn’t dilating fast enough. Then, doctors informed her she would need to have a second cesarean. Initially, she felt like a failure for not being able to have a vaginal birth. But she finds comfort in knowing she at least experienced labor.
In 2023, according to the World Health Organization, about one in three births in the United States were C-sections.
There are a few reasons why.
The overutilization of C-sections, Baker says, is because physicians are afraid of malpractice claims and lawsuits. While in training, she recalls physicians encouraging a C-section because “you never have to apologize when the baby comes out.” But this default decision has increased the risk of complications for patients.
“Not only is it a traumatic mental imprint that is forever left (on a patient),” Baker says, but they also face an increased risk of hemorrhage, infection, and postpartum complications. “There is a time where a C-section is needed … but this whole knee-jerk reaction to just do a C-section, if you’re unsure, needs to stop.”
Will I Die Giving Birth?
In 2023, when Dukes-Harris became pregnant again at 33, she was determined to do things differently with her birthing experience. To prepare for her daughter’s arrival, Dukes-Harris got a prenatal chiropractor and hired a team of three doulas and a home birth midwife.
“I can’t die giving birth,” she says. “My OB-GYN said that having a baby at 30-plus, over 300 pounds, is basically a death sentence.”
But her diagnosed anxiety kicked in and led her back to the hospital at 4 a.m.
“I physically prepared, but I didn’t mentally prepare for birth,” she says. “I was having an out-of-body experience.”
Doctors wanted to push for a C-section, but Dukes-Harris refused. Once her 6-foot-5 husband and midwife entered the room, she was able to successfully deliver her daughter vaginally. Now, after two birthing experiences that didn’t go exactly as planned, she created swishvo, a platform that connects patients and providers to access holistic health options.
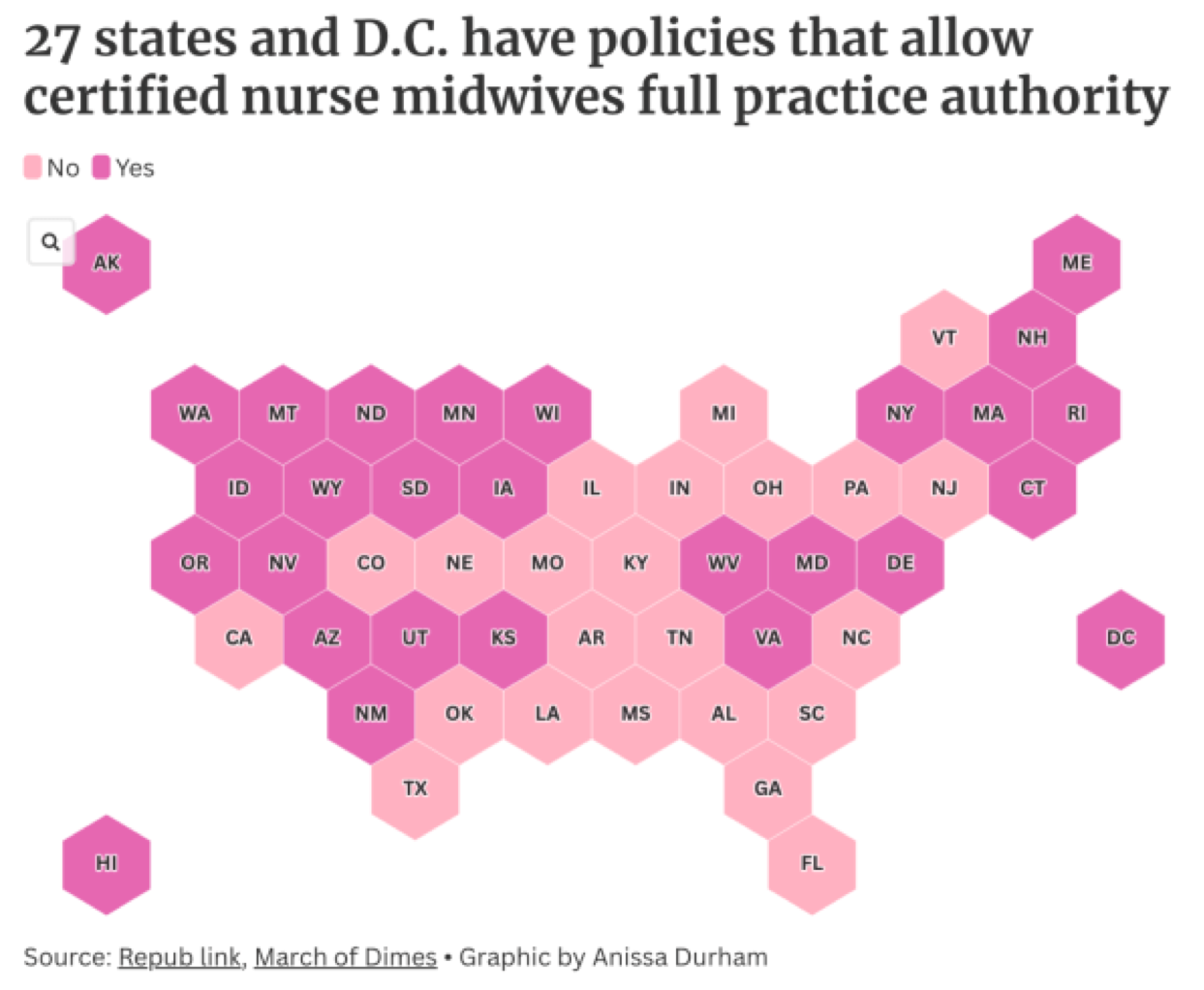 On a national scale, certified nurse midwives have been shown to improve birth outcomes for Black and American Indian, and Alaska Native communities. Currently, 27 states and D.C. have policies that allow certified nurse midwives full practice authority.
On a national scale, certified nurse midwives have been shown to improve birth outcomes for Black and American Indian, and Alaska Native communities. Currently, 27 states and D.C. have policies that allow certified nurse midwives full practice authority.
“Community-based birth workers, doulas, nurse navigators, lactation consultants, childbirth educators, we need all of that,” Baker says. “Our doulas are magnificent; they educate patients. We’re not able to do this by ourselves as physicians and midwives. We need a community of care for our patients.”
____________________________________________________________
Photo Captions:
Website Tags and Keywords:
Twitter Tags/Handles:





{kind=link}